Treatment Persistence and Healthcare Costs Among Patients with Rheumatoid Arthritis Changing Biologics in the USA
Adv Ther. 2017 Nov;34(11):2422-2435. doi: 10.1007/s12325-017-0617-5
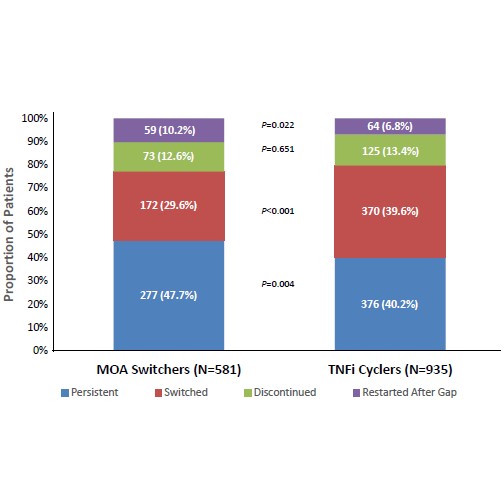
Updated treatment guidelines recommend the use of different mechanism of action (MOA) therapies earlier in the treatment course. Clinical studies have revealed that this approach may be better than TNFi cycling, and may be more cost effective.This study of Commercial and Medicare Advantage claims data showed that patients who switched MOA had higher treatment persistence and lower healthcare costs than TNFi cyclers.After the first TNFi claim, patients either cycled to another TNFi (n=935) or switched to a different MOA therapy (n=581). This included: abatacept, tociliuzumab or tofacitinib. Outcomes and costs were then examined for at least 1 year after this event. Median treatment persistence post-index was 366 days (95% Cl: 311-618) for MOA switchers and 279 days (95% CI: 257-306) for TNFi cyclers. The 1-year treatment persistence rate was 47.7% for MOA switchers and 40.2% for TNFi cyclers. The mean costs for 1-year post-index were significantly lower among MOA switchers than TNFi cyclers; RA-related cost ratios were 0.89; 95% CI 0.84–0.94 (P<0.001) and targeted DMARD cost ratios were 0.84; 95% CI 0.79–0.88 (P<0.001). Overall, these findings suggest that reimbursement policies that require patients to cycle before they switch to a different MOA my lead to suboptimal outcomes not just for patients but also for payers.