Safety and Efficacy of Upadacitinib in Patients with Active Rheumatoid Arthritis Refractory To Biologic Disease-Modifying Anti-Rheumatic Drugs (SELECT-BEYOND): a Double-Blind, Randomised Controlled Phase 3 Trial
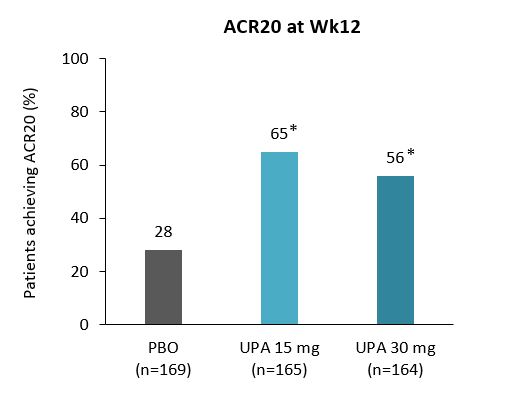
Upadacitinib (UPA) extended release formulation was effective in treating patients with moderate-to-severe RA with an inadequate response to bDMARDs.Phase 2 study data has shown that UPA is an efficacious and safe treatment for active RA.1,2 SELECT-BEYOND was a double-blind, long-term extension, Phase 3 study to assess the efficacy of UPA in patients with RA who were bDMARD-IR. The first 12-weeks of SELECT-BEYOND were placebo-controlled, with a double-blind period followed by an ongoing double-blind extension up to five years. This paper reports data from the first 24 weeks of this study. In addition to background csDMARDs, 499 patients were randomised (2:2:2:1) to receive either: extended-release UPA 15 or 30 mg QD, or PBO for 12 weeks followed by extended-release UPA 15 or 30 mg QD. Primary endpoints reported were ACR20 and DAS28(CRP)<3.2 at Wk12. Key secondary endpoints included proportion of patients achieving ACR20 at Wk1, ACR50 or ACR70 at Wk12, LDA, and HAQ-DI≥0.22 (MCID), change from baseline in DAS28(CRP), HAQ-DI, SF-36 physical component score, and duration of morning stiffness. Significantly more patients achieved ACR20 and DAS28(CRP)≤3.2 taking UPA 15 mg and 30 mg than PBO; for ACR20 significant differences were observed as early as Wk1. ACR responses were maintained up to Wk24, with ACR responses at Wk24 similar to those who received UPA from baseline and those who switched from PBO at Wk12. Incidences of AEs were similar for PBO and UPA 15 mg but higher for UPA 30 mg; the most common AEs reported were upper respiratory tract infection; nasopharyngitis, urinary tract infection, and worsening of RA. In this treatment-refractory population, UPA 15 or 30 mg QD resulted in rapid and significant improvements in clinical responses and functional and patient-reported outcomes. Both UPA doses had a similar efficacy, with a higher number of AEs reported for UPA 30 mg QD. However, a more comprehensive analysis is required once the Phase 3 programme is complete. 1. Kremer JM, et al. Arthritis Rheumatol 2016;68:2867–77.2. Genovese MC, et al. Arthritis Rheumatol 2016;68:2857–66.