Profil Lipidique et Effet du Traitement aux Statines dans des Études Groupées de Phase II et Phase III sur le Baricitinib
Taylor PC,
Kremer JM,
Emery P,
Zuckerman SH,
Ruotolo G,
Zhong J,
Chen L,
Witt S,
Saifan C,
Kurzawa M,
Otvos JD,
Connelly MA,
Macias WL,
Schlichting DE,
Rooney TP,
de Bono S,
McInnes IB
Ann Rheum Dis. 2018 Jul;77(7):988-995. DOI 10.1136/annrheumdis-2017-212461
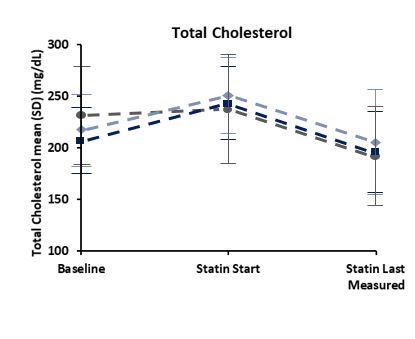
Baricitinib (BARI) was associated with increased lipid levels; baseline statins did not alter these profiles. The introduction of statins during treatment reduced total cholesterol and LDL-C.The use of anti-inflammatory drugs in RA patients has been shown to alter lipid levels and is associated with reduced atherogenic risk. Increases in lipid levels, specifically HDL-C and LDL-C, have been observed in Phase 2 BARI studies1.This study analysed data from seven randomised RA Phase 2/3 studies of BARI, assessing the effect of BARI and statins on lipid profiles. The impact of lipid alteration on cardiovascular disease risk, changes in risk scores and the association between LDL-C change and MACE was also assessed.Data were pooled into three sets; the 6-study PBO controlled set, the long-term BARI cohort and the all-BARI RA-MACE set. The data sets comprised Phase 2/3 BARI studies, and the long-term extension study, RA-BEYOND. Lipid levels for total cholesterol, LDL-C, HDL-C, triglycerides, apolipoprotein A-1, apolipoprotein B and GlycA were measured for each data set at baseline, Wk12 and Wk24. The effect of statins, at baseline or when initiated during the study, on the lipid profiles, and cardiovascular risk was analysed. Increases in circulating lipid levels were seen following treatment with BARI, which plateaued by Wk12 of treatment initiation; no significant change in the LDL:HDL ratio was noted. Baseline statin use did not modify the effect of BARI on lipids. Where statins were initiated during the study, total cholesterol and LDL-C returned to baseline levels, HDL-C remained elevated.Overall, BARI was associated with increased lipid levels which plateau by 12Wks. HDL levels did not decrease with statin therapy. Further evaluation of the effect of BARI on cholesterol and lipoprotein metabolism, and cardiovascular event rates during long-term treatment should help to elucidate these findings.1. Kremer JM, et al. Arthritis Rheumatol 2017;69:943–52.