Upadacitinib como Monoterapia em Pacientes com Artrite Reumatoide Ativa e Resposta Inadequada a Metotrexate (SELECT-MONOTHERAPY): Um Estudo de Fase 3 Duplo Cego, Randomizado, Controlado com Placebo
Smolen JS,
Pangan AL,
Emery P,
Rigby W,
Tanaka Y,
Vargas JI,
Zhang Y,
Damjanov N,
Friedman A,
Othman AA,
Camp HS,
Cohen S
Lancet. 2019 Jun 8;393(10188):2303-2311
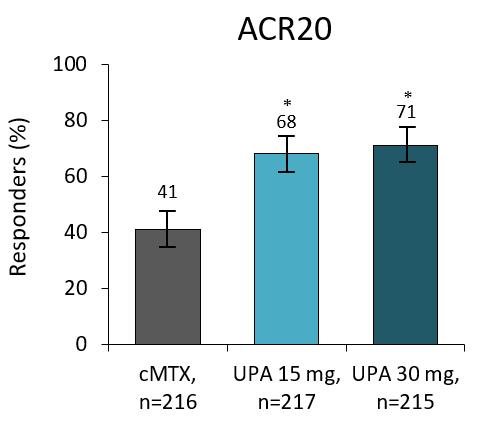
UPA monotherapy showed statistically significant improvements in clinical and functional outcomes versus continuing MTX in MTX inadequate-responder patients with RA. Despite its proven effectiveness and safety, many patients are unable to tolerate MTX due to its side-effects. Therapies that can be used without concomitant MTX therefore, have an important place in RA management. In previous studies, UPA has shown efficacy in combination with stable background csDMARDs in RA patients who are DMARD inadequate responders. This study evaluated the safety and efficacy of UPA monotherapy vs continuing MTX in patients with a prior inadequate response to MTX. Patients were randomly assigned 2:2:1:1 to receive either extended release UPA at 15 or 30 mg QD, or to continue the previous MTX dose as a blinded study drug, which was for administered for 14 weeks. Patients that stayed on continued MTX at Week 14 were switched to UPA 15 or 30 mg per prespecified randomisation assignment. Primary endpoints were patients achieving ACR20 and DAS28-CRP ≤3.2 at Week 14. Secondary endpoints included patients achieving ACR50/70, DAS28-CRP <2.6 and changes from baseline in DAS28-CRP, HAQ-DI and SF-36-physical component score and morning stiffness duration. At Week 14, 41% of patients receiving MTX achieved an ACR20 response (notable as a placebo arm), compared with 68% and 71% of patients receiving UPA 15 mg and 30 mg. DAS28-CRP ≤3.2 was attained by 19% of patients in the MTX group, compared to 45% and 53% in the UPA 15 mg and 30 mg groups. A greater proportion of patients achieved ACR20/50/70 and improvements in DAS28-CRP on UPA vs continued MTX from Week 2 onwards. AEs were reported by 47%, 47% and 49% of patients on MTX, UPA 15 mg and UPA 30 mg. Potential dose related AE included HZ, which were all reported as mild-to-moderate in severity. The benefit-risk profile of UPA monotherapy provides a further treatment option for patients who are intolerant to MTX or to those who prefer treatment without the need for concomitant csDMARDs.