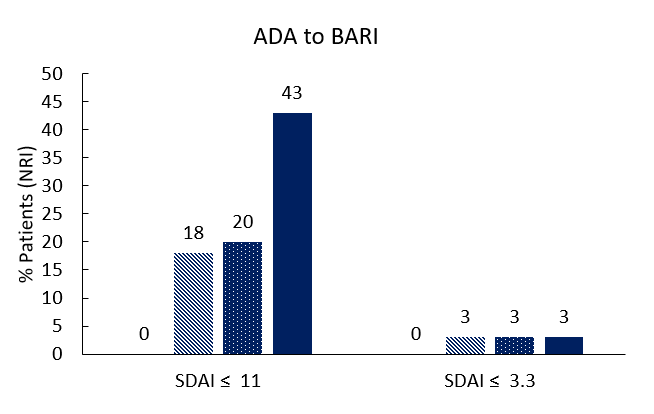
Desfechos Clínicos em Pacientes que Trocaram de Adalimumab para Baricitinib devido a Falta de Resposta e/ou Desenho do Estudo: Fase 3 em Pacientes com Artrite Reumatoide
Tanaka Y,
Fautrel B,
Keystone EC,
Ortmann RA,
Xie L,
Zhu B,
Issa M,
Patel H,
Gaich CL,
de Bono S,
Rooney TP,
Taylor PC
Ann Rheum Dis. 2019 Jul;78(7):890-898.
Switching from ADA to BARI without a lengthy washout period can be executed with acceptable safety and tolerability and was associated with maintained disease control. Switching therapies in RA is commonplace in myriad scenarios including inadequate responses, intolerances and patient preference. Assessing the safety and efficacy of new treatments such as BARI, in the context of use as a replacement therapy, is beneficial. A previous study (RA-BEACON) has demonstrated that safely switching from ADA to BARI was achievable, albeit with a four-week washout period. The aim of this study was to evaluate clinical outcomes in patients who changed from ADA to BARI without a lengthy washout period, during both RA-BEAM and RA-BEYOND.Patients in RA-BEAM were assigned 3:3:2 to: PBO, BARI 4 mg, or ADA 40 mg. At Wk16, patients could be rescued from any arm to BARI 4 mg and at Wk24, all PBO patients were rescued to BARI 4 mg. After completing RA-BEAM, patients could enrol into the LTE study, RA-BEYOND, whereupon all patients switched to BARI regardless of their response to previous ADA treatment. Efficacy and safety were assessed based on the proportion of patients achieving LDA, remission, SAEs, HAQ-DI, and patients’ assessment of pain across both studies. Of the 1305 patients that received treatments, 7% of BARI and 12% of ADA patient groups were rescued to BARI during RA-BEAM. Consistent with the prior findings of RA-BEACON, patients benefitted clinically with significant improvements in mean CDAI, SDAI and DAS28-ESR at Wks 4, 8 and 12 post rescue. Sustained improvements in pain and physical function were observed 4 weeks post rescue however during RA-BEAM; EAIRs, SAEs and AEs leading to discontinuation were numerically higher in patients who continued BARI.In patients initially treated with ADA, mean CDAI, SDAI and DAS28-ESR showed statistically significant improvements through 24 weeks of RA-BEYOND, after switching to BARI 4 mg. At Wk24 of the LTE, both BARI and ADA groups had similar outcomes related to pain and physical function. Infections and serious infections were also similar in both groups. Adverse event data from the period immediately following the treatment change suggest transitioning from ADA to BARI without a lengthy washout period can be executed with acceptable safety and tolerability.